OVERVIEW
The
An imposed challenge for us is to determine “how” to measure significant performance outcome and thus accord the title of “The Healthiest Community in
I have been seeking that elusive “Rosetta Stone” for almost six years now. Reading literally hundreds of books, scouring the internet (almost a thousand papers and articles) and I have yet to find any menu of measurement that satisfies this goal. Therefore, I have come to the conclusion WE will measure WHAT ever is important to our goals of Wellness and in following pages we will discuss HOW. But first…….
THE NATURE OF A CCRC
Consider the demonstration community type we are using as the first application for the focus of the
The three major categories of living accommodations are uniquely different from each other. They are: Independent Living, Assisted Living, and Skilled Nursing Care. Each of these continuums has at the basis, a uniquely targeted program calibrated to meet the needs of their constituents.
The clinician with stewardship over a population of the “elderly / feeble” has an understandably strong need to be constantly aware of the resident/patient’s vital signs. However, the wellness director creating programs for the active seniors in the independent living program of the community has more of a need to take measure of the “vitality” signs or as we would say, the “
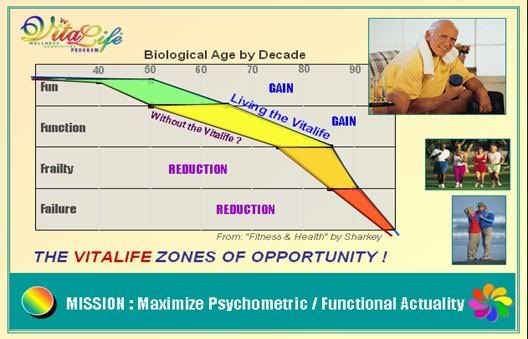
These two continuums serve different people at four different levels of capability, as indicated in our graph. The categories are: 1) Fun, 2) Function 3) Frail, and 4) Failure.
THE NATURE OF MEASUREMENT OR TESTING
Measuring is not useful unless it benefits an individual and a process. Measurement used for health screening has approximately three levels:
1. Common Health Profile Screening employs a denominator measure of Respiratory, Cardiac, Nervous and Circulatory systems as well our growth measures of weight and height. These basic health screening tests and diagnostics can be performed relatively quickly, are general in nature, and are the lowest cost of the diagnostic family of screening and testing. These are used to provide baseline data for a patient, so that they can be benchmarked in the future relative to them and the population-at-large.
2. Follow-up Testing. This testing is more targeted, depending upon the Primary Screening Results. It is more specified than a common health profile screening, often more expensive. Both of these first two testing programs are basically seeking morbidity indicators, and are employed when maintaining a body that is more often than not in declining health.
3. Performance Testing, such as that utilized by competing athletes, is seeking to obtain higher levels of vitality and thus capability. Their goal is to seek and accomplish “Personal Best” or “Category Best” in whatever endeavor they have chosen to become accomplished.
TWO ENDS OF THE CONTINUUM
In a CCRC, a 68 year old man, may choose to work out in a gym to improve his upper body strength, which helps to compensate for the natural loss of strength occurring with the natural aging process. A 72 year old woman may be taking piano lessons as a mental exercise to help her maintain her memory functions and also to defer the threat of one of the many stages of dementia or Alzheimer’s.
A man or woman of any age, suffering from loss and loneliness, after having suffered a significant personal loss such as a death of a family member, could experience significant depression. Additionally, he or she may experience mental stress disorders which require intervention of another kind of treatment and therefore measure. In this scenario, just what do you measure to ascertain the welfare of the patient? To begin, patient could be asked in a questionnaire the answer to a question requiring self-reflection and subjectivity such as, “are You Happy or Sad, and Why?”
NO ONE SIZE FITS ALL
Obviously, there is no “one size that fits all.” When examining the measure of communities or small towns designated annually by the AARP, Rand McNally, or others that serve the aging senior demography, we find they are open in sharing their measurement categories. They each differ due to the understandable lack of empirical measure to enable one to be proven “right” and another “wrong.” They share their logic with the reader and offer some measure but a largess of subjective and anecdotal data to make their case. This prompts the reader to take the responsibility of either agreeing or not with the study and /or its author.
THE VITAL LIFE COMMUNITIES SHALL MEASURE ANY NEEDED ACTIVITY
This is any data that is needed and has been accepted as a common standard of measure for those specialties of concern as required by our constituents. There will be different standards for instance of the quality, and nutritional food content served, relative to the diabetic, versus the sufferer of arthritis.
There will be a “personal best” for an 88 year old woman using a walker and working her way back to independent ambulation after hip fracture surgery, as there will be for a 68 year old man who is trying to increase the fractional additives of the weights he will be trying to bench press.
INDIVIDUALLY WE WILL MEASURE . . .
In all cases, the goals are the same. As you look at the chart above, the basic tenants of the
AS A GROUP WE WILL MEASURE…
Each community will employ their own measurements to define resident satisfaction and maximum benefit of symbiotic interfacing. For those who have no measure or find the academic and statistical scientific methodology too daunting, we offer the VCWP formula for measure social transaction as:
CxDxQ= S < 3
Wherein: C = CONTACT: Numbers of persons in group connected
D = DURATION: Duration of time (in minutes) group stays involved
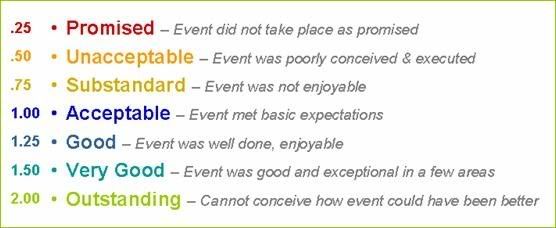
Q = QUALITY: Subjective satisfaction rating by participants in activity being measured (see chart below)
S = Social Transaction
A RESIDENT WILL MEASURE
In the end, the outcome that matters most is resident participation. You can have a powerhouse of talent within your staff and resident community, but without providing the venues that will allow them to engage and focus on initiatives that matter, then the potential for both resident and community is wasted.
It becomes imperative that we ensure the engagement of the residents; their satisfaction is paramount to both the vitality of the community and to them. They are unusually above the common mold or they would not have chosen your community or have had the resources to afford your offering.
So in the end, it is the responsibility of the community to offer vital activities that will enhance the vital life of the resident and therefore the vitality of the community. There is no shortage of evidence describing the nature and the material content of programs designed to provide almost any outcome desired.
MEASURING THE HEALTH AND VITALITY OF THE COMMUNITY
As stated earlier, measuring the vitality and well being of residents from a biophysical sense is relatively well developed within our culture in terms of diagnostics and corresponding relevance. In the triad of “mind, body, and spirit,” we have as a society developed fairly sophisticated bodies of knowledge such that any known malady has an intercessory or preventative program to mitigate its threat to the health of the body.
Regarding physical fitness, there is no shortage of aerobics classes, balance, fitness, strength training or other bio-physical programs, in most any community. It is in the realm of “mind and spirit” wherein the deficit often occurs. Often times “lifestyle” in a community sometimes seems institutional with a mild sense of benign incarceration, rather than life being meaningful, serendipitous and liberating.
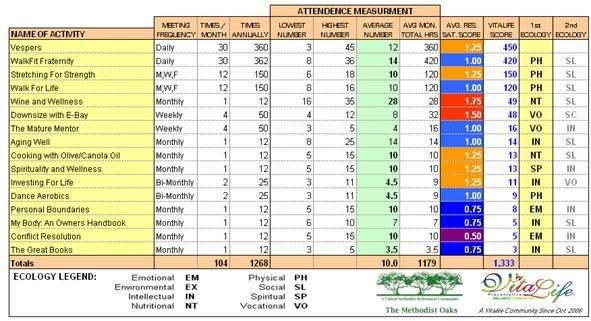
What we are short on is motivational techniques and the balancing of application of programs relating to mind and spirit. The chart below shows how one can monitor the “balance” of the program offerings within a community not just quantitatively, but “qualitatively.” This is the measure that truly establishes the currency of value that separates one community from another.
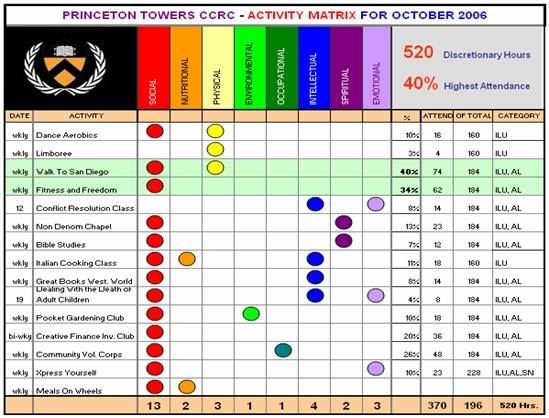
The ACTIVITY MATRIX shown on the previous page represents a log of just some the activities for one month within a fictitious Vital Life Community that is employing the Vital Life program. This “mock” chart was created to demonstrate how to compile data so that it is useful, while providing direction and guidance.
In the matrix, one can readily see the utilization of the types of programs, the patronage, the continuum sectors participating, and the resident satisfaction. You will note that in this community, they could use more programs that have to do with the human ecology spectrum subjects of the “environmental”, “spiritual” and “occupational” genres.
They have very good participation in the “physical” fitness realm of walking and general fitness classes. This could be because the perception of the residents is that if they participate in these classes, it will provide the best investment return for their most precious and finite asset, their time.
VARIETY IS THE SPICE OF LIFE; ENGAGEMENT IS THE “BEEF!”
Just as in our favorite cities that we like to visit, our favorite communities are ones that have a wide variety of activities that can provide people with varied taste “options.” The key, however, is ENGAGEMENT. Individuals and couples will only be satisfied with being observers initially, until the “newness” wears off. Then they will be anxious to participate and become a part of the “buzz of the hive!”
To successfully accomplish the “ENGAGEMENT” portion of the community, the activities program is the first element that must be mastered. Both Motivation and Engagement can be programmed by an astute Wellness Coordinator or Program Director.
This is where the “art” of being a successful motivator comes in, and this is where the survey response that highlights the “SATISFACTION QUOTIENT” shown on page 4 comes in. In almost all occasions, a score of 1.25 to 1.75 will be realized only if there is an embedded or hosted “mixer” component. By this we mean making people feel comfortable enough to engage with strangers in hopes of them getting to know them and make new friends. Many new residents have lost all or most of their former friends and colleagues; therefore, they are weaker because of a thinning support group.
This “mixer” motivational technique is the social secret of any good hostess. She knows her guests, knows what they are interested in, and introduces them “to” others with enough information that they have common ground for both respect, and conversational exchange opportunities.
HELPFUL HINT:
Techniques on “breaking the ice” and “motivating residents” will be found in both the VITAL NATION net programs: the BBS, and the BLOGS. Go to http://www.vitalifecommunity.com/ and then click “forums” to be taken to the BBS.
BREAKING THE MOLD IN MEASURING OUTCOMES
Would you say that getting a resident in Assisted Living or Skilled Care to participate in a “Walk to
I encourage you to read one Vital Life Community member’s report on her successful motivational techniques. She was able to motivate a marginally ambulatory resident to participate with the more mobile residents on a “Cross Country [walking] Conquest” program. Go to: http://vitalactivities.blogspot.com/
ONE SIZE DOES NOT FIT ALL
Each resident will have differing needs depending upon their health and ability. A resident who is non-ambulatory and suffers from chronic arthritis will have different primary goals than another resident that is actively mobile. A well resident might seek a broader dimension of experiences depending upon their make-up and interests.
Each community will have at any given time a “Dynamic Need” status. Depending upon the resident population, certain initiatives will be received more readily than others.
If residents feel that the community will genuinely take their feelings into account when considering CCRC program implementation, they will give honest feedback that will benefit the effectiveness of the programming. This way existing programs can be tweaked such that they will become continuously more relevant to the resident population, simply by asking them and responding in kind through interviews and surveys.
It is important to not only survey the residents but critically important to “respond” to the survey results with appropriate changes or mid-course corrections to aspects or nuances of your existing programs. Having a program alone, will not result in resident satisfaction, indeed it could engender criticism. However, in the residents’ minds, squandering their precious time by operating a program that is not what it should be or one not satisfying to them is not acceptable.
HOW DO WE CONTINUALLY MONITOR AND MODIFY OUR PROGRAMS?
The Vitalife “Resident Satisfaction Survey” is quite useful, to accomplish this end and quite easy to understand. It takes each resident only minutes to fill out, is simple to process and over a period of time will offer a clear diagnostic of your program suite.
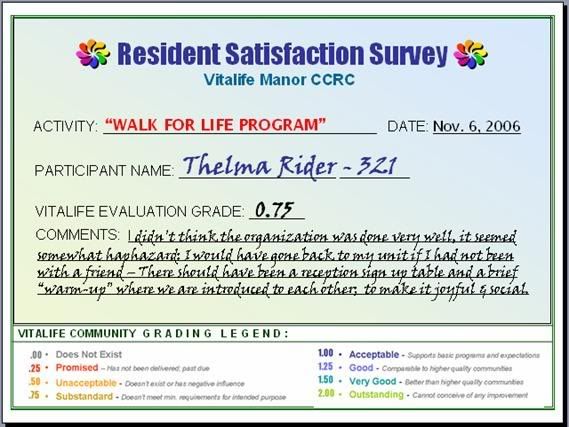
Thelma Rider (above) did not give a good score to the walking program. She expected a program to have an organization that would facilitate “partnering” or facilitation. Her survey results do not indicate that directly. She complains (and gives a low score) because when entering the lobby where the walking program around the grounds was to begin, it was not evident among the varying clusters of people just who were walking and who were not. She wanted to walk “with” somebody, and when the group just started walking out the door, she followed but did not feel a “part of it.”
A follow up phone call would have added “the rest of the story.” Thelma was hard of hearing and could not hear the walk leader’s (a petite woman not readily visible in a crowd) instructions to the crowd. She would have responded better to a “visible” cue such as an easel indicating that this was the starting point and each person should sign in and contact the “walk leader” wearing the red hat.
A follow-up phone call would accomplish two things; 1) Advise Thelma how to better facilitate immersion into the program, and 2) indicate to the “walk leader” that a visual cue was needed to help orient new residents as to the protocol.
The next walk session, the “walk leader” actively seeks Thelma out and pairs her up with another person who “knows the ropes” and who is known for talking loudly at all times. Thelma then upon completion of her walk fills out another Survey and her score reflects greater satisfaction, and both Thelma and the Community have gained because now the program is better and more resident based.
The Resident Surveys should be an important part of the continuing methodology of listening to the “buzz of the hive.” Some residents will not want to fill out a survey each time they finish a walk, it will become tedious. That’s O.K.; this means they are relatively satisfied. But the population should be made aware that the Resident Survey forms (RS Forms) are ALWAYS available at the location of the event, and at the end of each event the leader should remind “those who want to, don’t forget to fill out your forms!”
Upon completion of even three months of using RS Form system, dramatically useful information will start to materialize. Quarterly, the Vitalife Scorecard should be available to the residents to show how they have graded various programs and activities. More importantly this will show them how their satisfaction has increased due to an alert, caring and responsive program or wellness director’s efforts.
RESIDENT SATISFACTION Forms
From these RS Forms combined with a “sign-in” sheet at every function a mosaic of the activities of the community begin to reveal several things:
1. The diversity of the program (diversity is crucial to wellness)
2. The quality of the programs from the resident’s view point
3. The favorites of the community
WHY ARE THESE THREE COMPONENTS IMPORTANT?
DIVERSITY
Diversity is the key to a “balanced” program, ensuring that all residents with all proclivities have something that allows them to participate “socially” within their own community. This allows them grow, engage, learn, and to be exposed to new stimuli that may change their lives. Meeting one new person, who is passionate about one aspect of life may change the life of a new friend, and a person who never held a paint brush in his life could discover the hidden painter talent within himself.
QUALITY
Quality is a subjective aspect in that it takes on a new meaning with each individual. Resident satisfaction is allowing you to precisely “tune” programs that have otherwise no precise “tuning controls.” The residents TELL YOU where and what the controls are.
FAVORITES
Favorites are important because using the 80/20 rule. Every effort must be employed, especially when the assets of facilities, time, and money are finite, to maintain and improve key programs that pull the residents out of their place of abode and into the social mix of the community. Socialization will keep our residents vital and looking forward to living – living in your community, and this will in turn enhance their outlook on life!
Plan, implement, measure, modify (PIMM): the PIMM method must be the continuing cycle of vitalizing your community. Data delivered to you via the RS Forms, and information extracted by you, via Survey Follow-up (SF) should be charted, selectively shared, and employed to create a Vital Community.
The PIMM process is the MEASURE of a successful community and the measuring process, with the appropriate response and feedback is the KEY to a more Vital life. Fully Human and Fully Alive – That is the measure of vitality.

No comments:
Post a Comment